









Story highlights
Prescriptions for opioids rose from 76 million in 1991 to 207 million in 2013
Overdose deaths from prescription opioids more than tripled in the past 20 years
Insurance companies lose an estimated $72.5 billion annually because of opioid addiction
The latest fighters in the opioid addiction epidemic aren’t addicts-turned-activists, cops or even addiction counselors. They are health insurance companies.
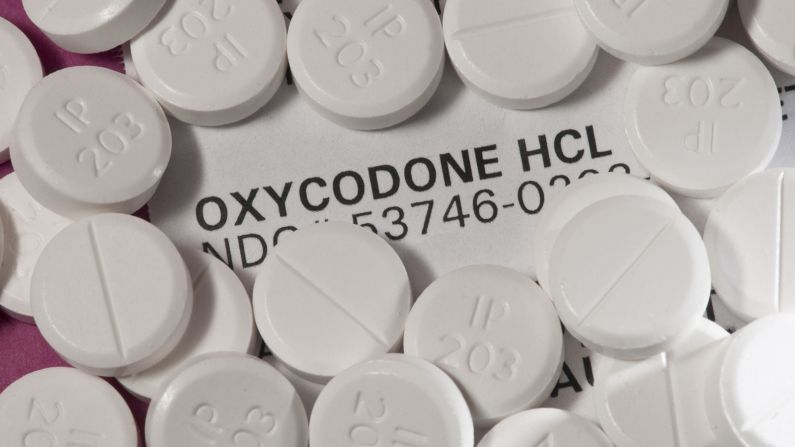
Cigna, which insures about 14 million Americans, has become the latest major health insurance company to take measures to combat the staggering opioid addiction numbers and deaths, targeting what many feel is feeding the problem: overprescribing of prescription painkillers such as oxycodone, hydrocodone and morphine.

Companies such as Aetna and Blue Cross Blue Shield have taken similar measures over the past several years to prevent deaths and keep addiction numbers from going up. It also makes good business sense: One researcher points out that the cost to public and private insurance companies of prescription painkiller abuse, treatment and “diversion” (when patients sell the medication instead of taking it) is an estimated $72.5 billion a year.
And because these insurance companies play a big financial role in health care, they might be able to make some of the most impact, says Dr. Andrew Kolodny, a senior scientist at Brandeis University’s Heller School for Social Policy and Management.
“They’re paying the bills,” Kolodny said. “They’re paying for the medicines that people are getting addicted to. They’re paying for the doctors’ visits where people are getting medicines prescribed. They’ve got quite a bit of influence in this.”
Making use of patient data at their fingertips
For years, Cigna, like other major health insurance companies, has had access to prescription information for its customers. Any time you fill a prescription using your insurance, the company knows about it. Part of Cigna’s new measure will be to flag those customers who are deemed high-risk – either for getting large amounts of opioid medicines, for getting narcotics from different doctors or for being on the medicines for a long time – and getting in touch with those customers’ doctors.
“We reach out to the doctors who are prescribing and let them know that this history exists,” said Dr. Doug Nemecek, chief medical officer for Cigna’s behavioral health business. “We ask (the doctors) to look at the history themselves and make a decision: Is it appropriate, or is it not appropriate?”

If the doctor believes that addiction may be an issue, the insurer can help get him or her to talk to the patient about treatment options. If the doctor feels the patient still needs to be prescribed long-term narcotics, Cigna can limit where the patient is able to pick the medicine up and which doctors are able to prescribe narcotics to them, so that the doctor is able to closely monitor whether that patient seems to be needing more and more painkillers.
But if a patient goes to other doctors or pharmacies asking for narcotic painkillers, Cigna cannot tell the pharmacy not to fill a prescription; the insurer would simply not pay for it.
There are already databases that look at what kinds of prescriptions a patient has been filling – called Prescription Drug Monitoring Program databases – and they generally pull together data in each state. But it’s difficult for some doctors to know what prescriptions patients are filling in other states.
As Cigna points out, only about 20% of doctors actually consult these databases, so the insurer will take it upon itself to point out to doctors which patients may raise red flags.
The company also wants to make sure “medication-assisted therapy” – which combines therapy with addiction treatment medicine such as Suboxone – is available to those who need it.
How similar programs have fared
Cigna is not the first health insurance company to turn to these measures. In 2012, Blue Cross Blue Shield of Massachusetts – which serves about 3 million customers in the state – started a similar program.
Dr. Tony Dodek, the associate chief medical officer for BCBS Massachusetts, saw that 1% of the its customers – or about 30,000 people – were getting first-time prescriptions for long-acting narcotics.
“It sounds like a low percentage, but it’s a lot of people,” Dodek said.
BCBS Massachusetts made changes. If a patient is getting more than 30 days worth of prescription painkillers, the doctor has to get prior authorization from the insurance company. The doctor will assess the addiction risks for that patient. Oftentimes, patients are required to sign “treatment plans” in which they acknowledge that they know about the risk of addiction with opioid medicines and promise to get these prescription painkillers from only one doctor.
BCBS Massachusetts said it’s eliminated about 21.5 million “doses” of opioid medicines in its community. And in three years of the program, it’s gotten only one complaint.
“We’ve even received a few notes from some members thanking us, because if it wasn’t for the program, they wouldn’t have gotten help,” Dodek said.
Aetna, which serves nearly 47 million customers, has been monitoring its claims database for signs of “above-normal use” in prescription painkillers and a large number of emergency visits. From 2010 to 2012, the company was able to decrease the number of opioid prescriptions by 14%.
Cigna, like these companies, has been monitoring customers for possible signs of addiction or fraud for several years; the difference now is that it will expand the program to include patients who may be at risk for being over-prescribed.
‘The target is way too low’
For those who see and treat Americans struggling with opioid addiction every single day, these measures are not enough.
Cigna aims to reduce the number of opioid prescriptions written to its customers by 25%, back to the number of prescriptions that were being written in 2006, which the insurer calls “pre-crisis.”
For Kolodny, who is also director of Physicians for Responsible Opioid Prescribing, the crisis actually started about a decade earlier. Data from the National Institute on Drug Abuse show that the number of prescriptions for opioid medication started skyrocketing in 1996.
Join the conversation
“If that’s what they’re targeting, that’s a big a mistake,” Kolodny said. “I think the target is way too low. I think they should be going for much more significant reduction.”
Kolodny also points out that the databases that insurance companies use to track what medicines their customers are getting show only prescriptions that are paid for by the insurance company.
“For people who are addicted or diverting, they’ll usually use their pharmacy benefits for the first prescription and pay cash after that simply because, even if they tried to use pharmacy benefits, they would get denied. Paying cash is very common.”